
Study design for adult upper limb spasticity
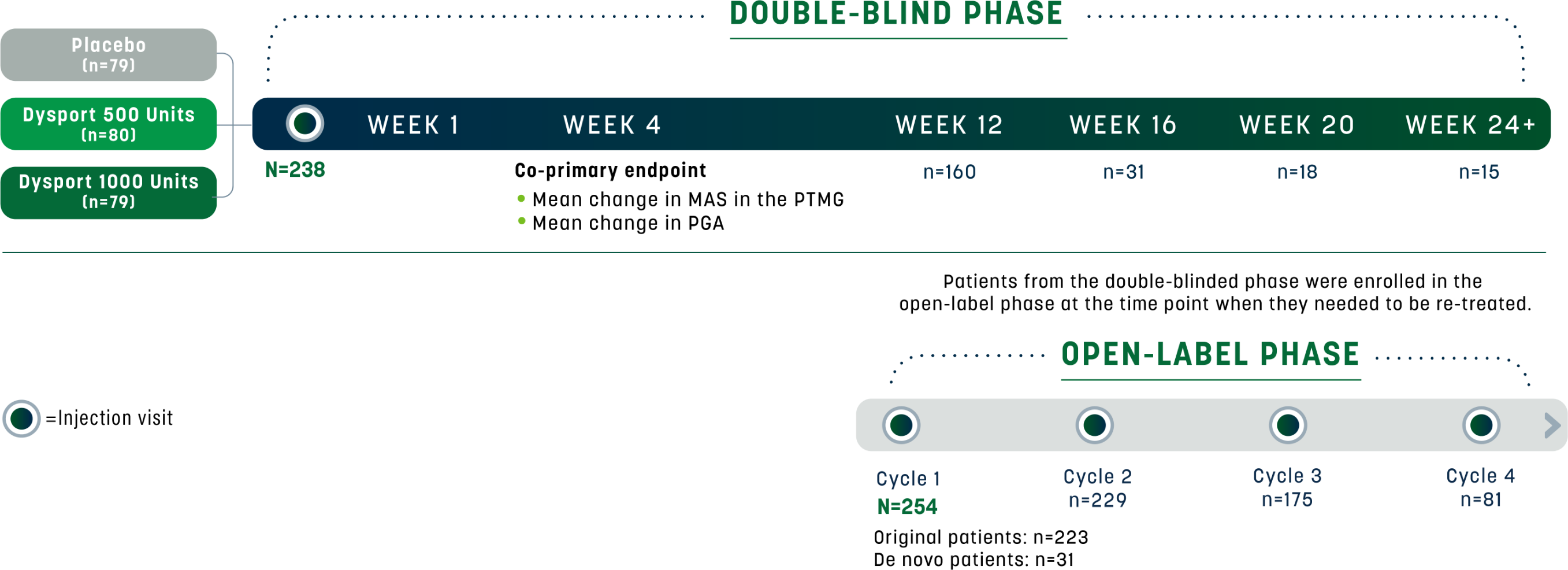
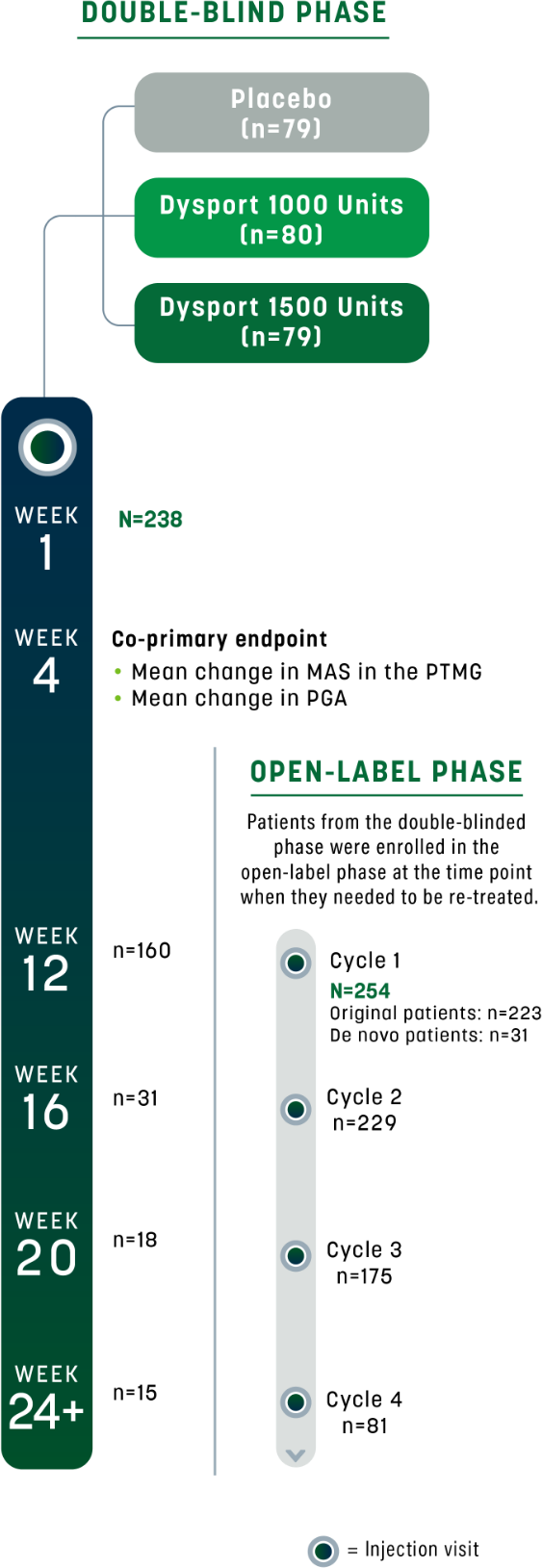
The efficacy and safety of Dysport were evaluated in a randomized, multicenter, double-blind, placebo-controlled study in 238 adults with upper limb spasticity (ULS) who were at least 6 months post-stroke or post-traumatic brain injury. Modified Ashworth Scale (MAS) score was ≥2 in the primary target muscle group (PTMG) for toxin-naive patients, or ≥3 at least 4 months after the last injection for toxin non-naive patients; and spasticity angle ≥10 degrees in the PTMG.1,2
The co-primary efficacy endpoints were mean change in MAS score in the PTMG (elbow, wrist, or finger flexors) and Physician Global Assessment (PGA) of response to treatment between baseline and Week 4. MAS score at baseline (mean [SD])1,2:
- Placebo: 3.9 (±0.4)
- Dysport 500 Units: 3.9 (±0.5)
- Dysport 1000 Units: 3.9 (±0.4)
Follow-up assessments occurred at Weeks 1, 4, and 12; follow-up visits were also permitted at Weeks 16, 20, and 24 as needed for re-treatment. After 3 months of on-study treatment, patients were given the opportunity to continue open-label treatment with Dysport. In the open-label phase, patients who were permitted entry from the double-blind study were offered Dysport for ≤4 treatment cycles at ≥12-week intervals. A total of 254 patients were enrolled.2
Study design for adult ULS1,2
Study participants included both toxin-naive* and toxin non-naive patients.2


AUL – MAS in the PTMG


- Patients received Dysport 500 U, Dysport 1000 U, or placebo; co-primary efficacy variable was muscle tone assessed by the MAS at the PTMG at Week 42
- MAS score at baseline (mean [SD]): placebo, 3.9 (0.4); Dysport 500 Units, 3.9 (0.5); Dysport 1000 Units, 3.9 (0.4)2


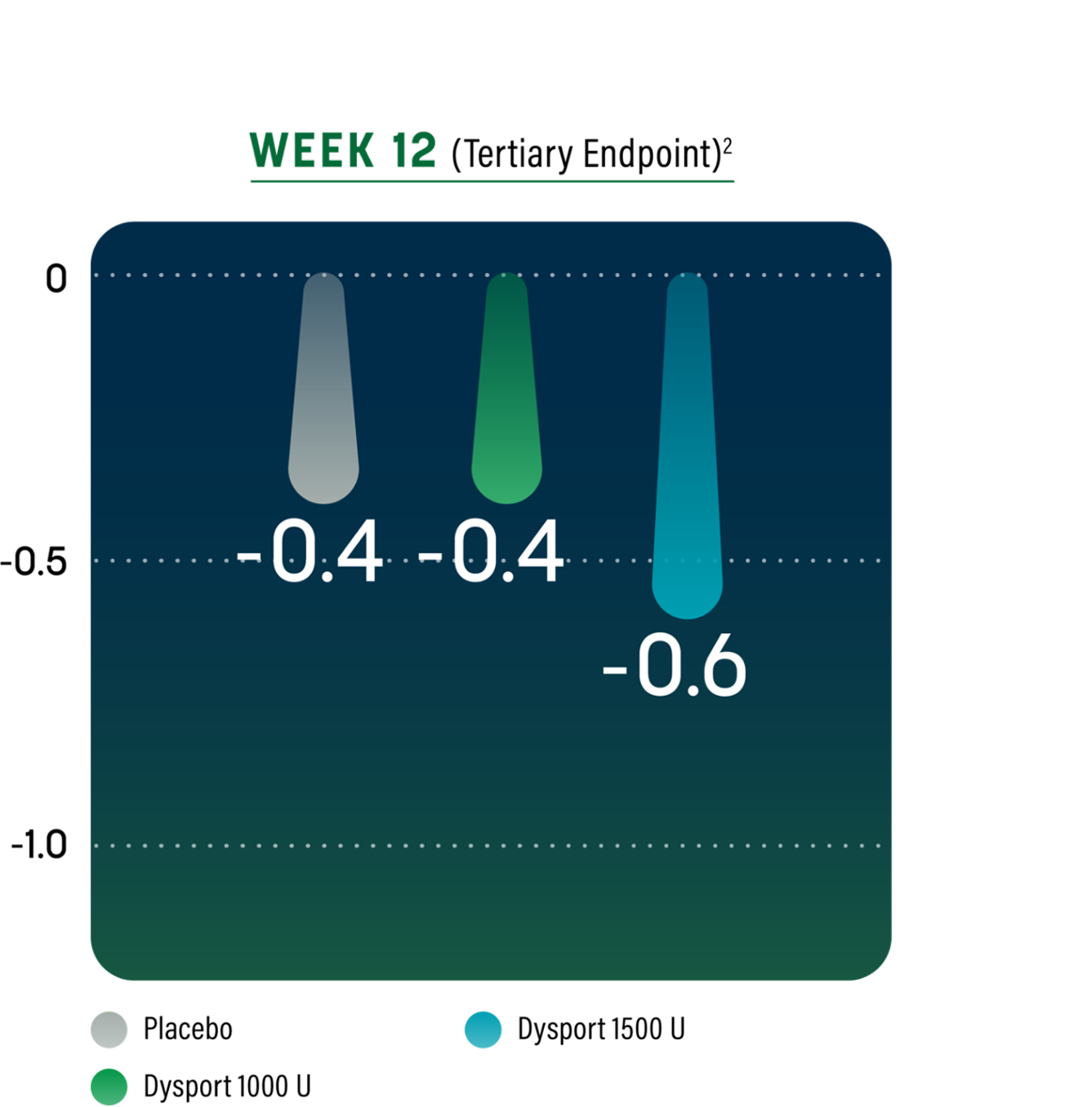
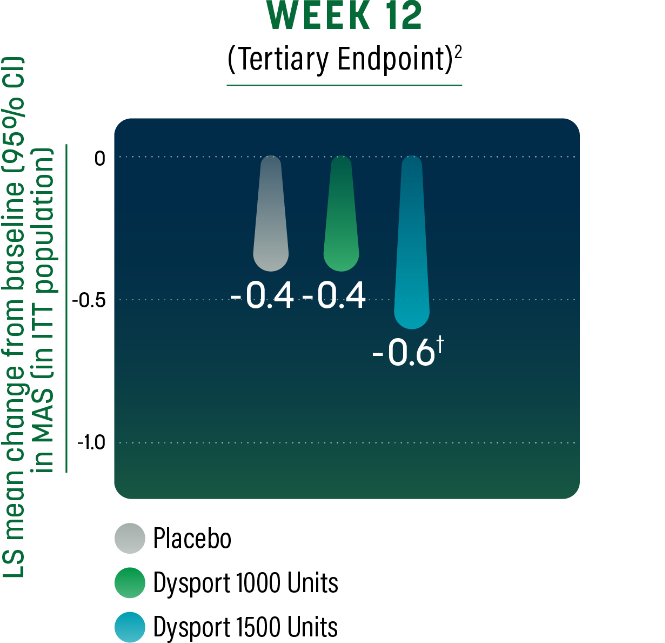
Study Limitations: Week 12 results may represent chance findings, as multiplicity adjustments were not applied; therefore, the results should be interpreted cautiously.
- Change in MAS in the PTMG through the minimum re-treatment time of 12 weeks2
CI=confidence interval; ITT=intent-to-treat; LS=least squares.
AUL – Physician Global Assessment
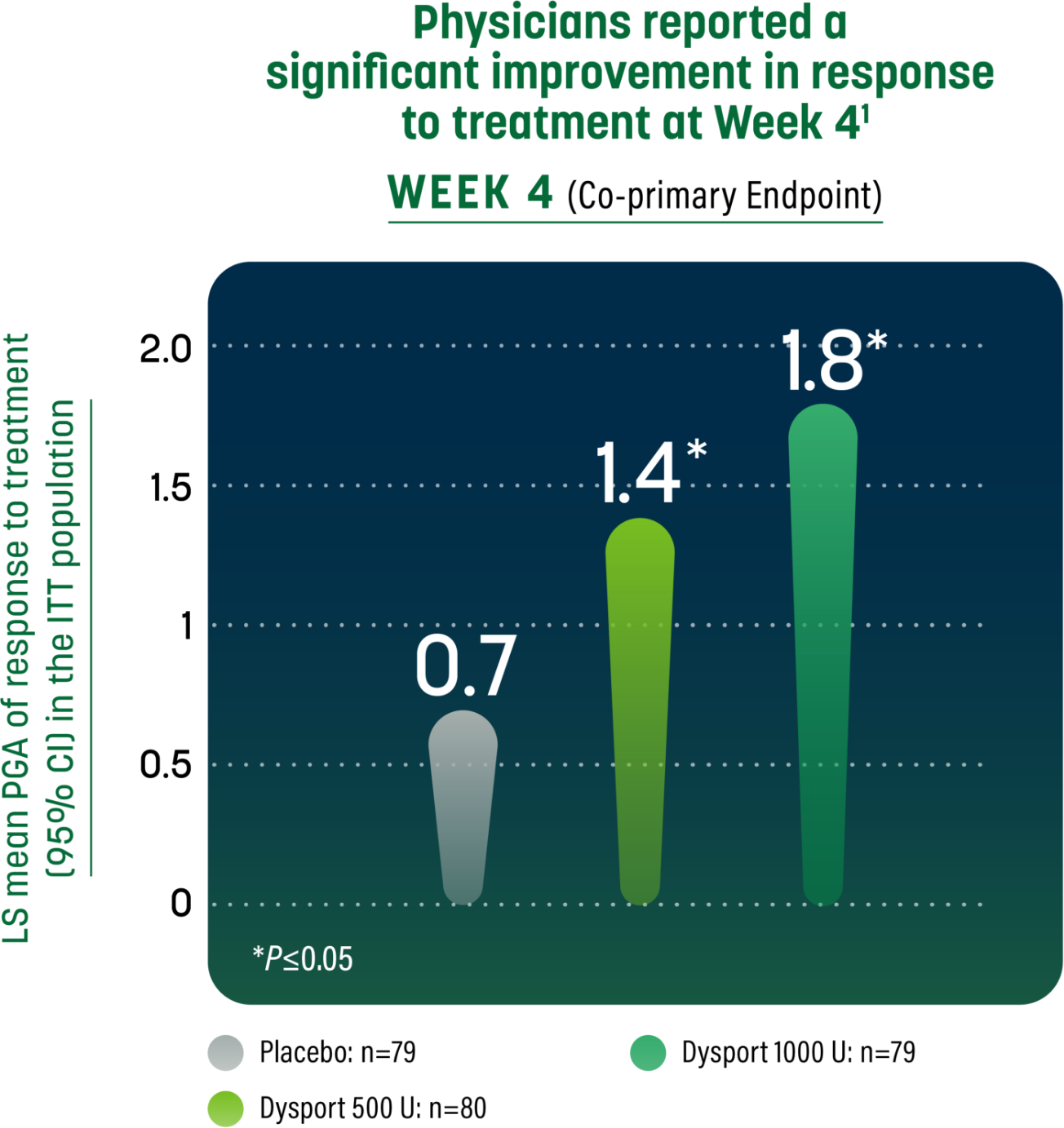
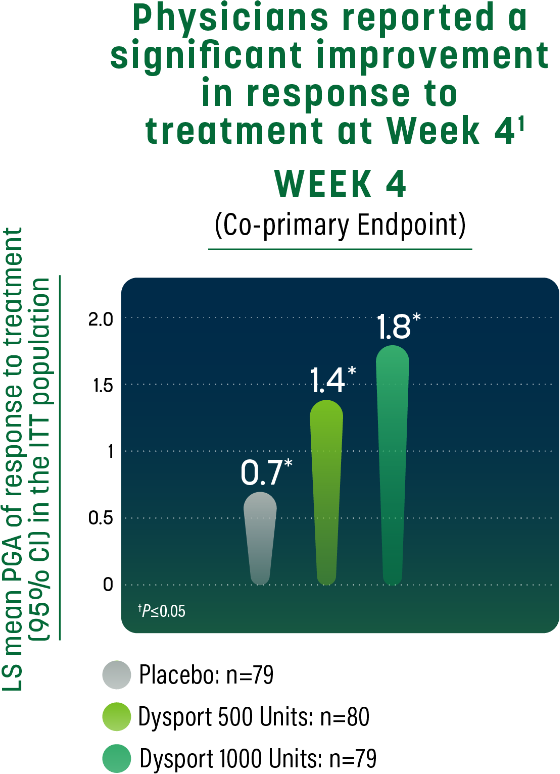
- Patients received Dysport 500 U, Dysport 1000 U, or placebo. Co-primary endpoint was improvement in response to treatment as assessed by PGA or response to treatment at Week 41
- PGA based on 9-point rating scale from -4 (markedly worse) to +4 (markedly improved)2

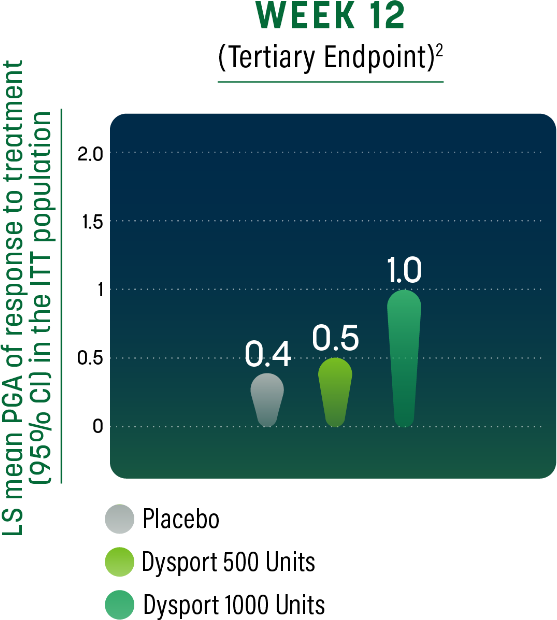
Study Limitations: Week 12 results may represent chance findings, as multiplicity adjustments were not applied; therefore, the results should be interpreted cautiously.
- Response to treatment in patients receiving either dose of Dysport was observed through the minimum re-treatment time of 12 weeks2
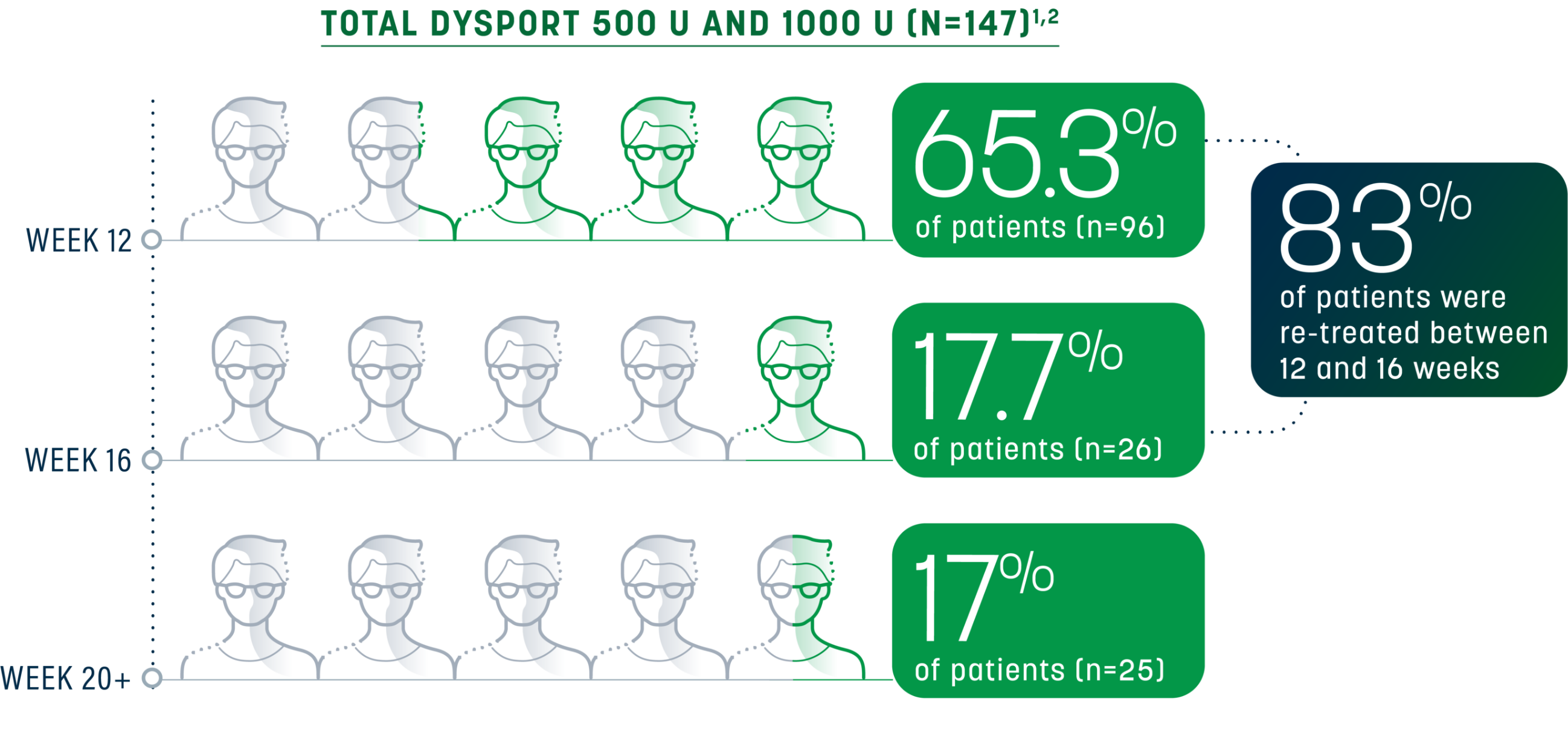
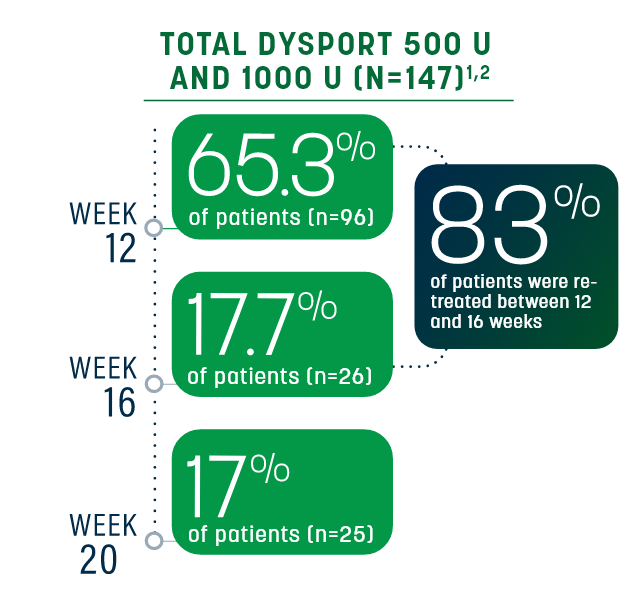
Sustained relief beyond the minimum time to re-treatment
Re-treatment was between 12 and 16 weeks for 83% of patients (Dysport 500 Units, Dysport 1000 Units; n=147); however, some patients had a longer duration of response (20 weeks)1,2
Re-treatment criteria
In the pivotal trials for adult spasticity, need for re-treatment was determined by2:
- No longer demonstrating a decrease from baseline of ≥1 grade in MAS score in the PTMG
- No improvement in PGA (ie, a score ≤0)
- No signs of unacceptable safety risk for next treatment cycle
Investigator discretion (based on efficacy and safety criteria) determined the need for re-treatment in patients demonstrating a decrease from baseline of ≥1 grade in MAS score and/or improvement in PGA (ie, a score ≥1).2
Repeat Dysport treatment should be administered no sooner than 12 weeks after the previous injection.1
Learn more about Dysport for adult ULS

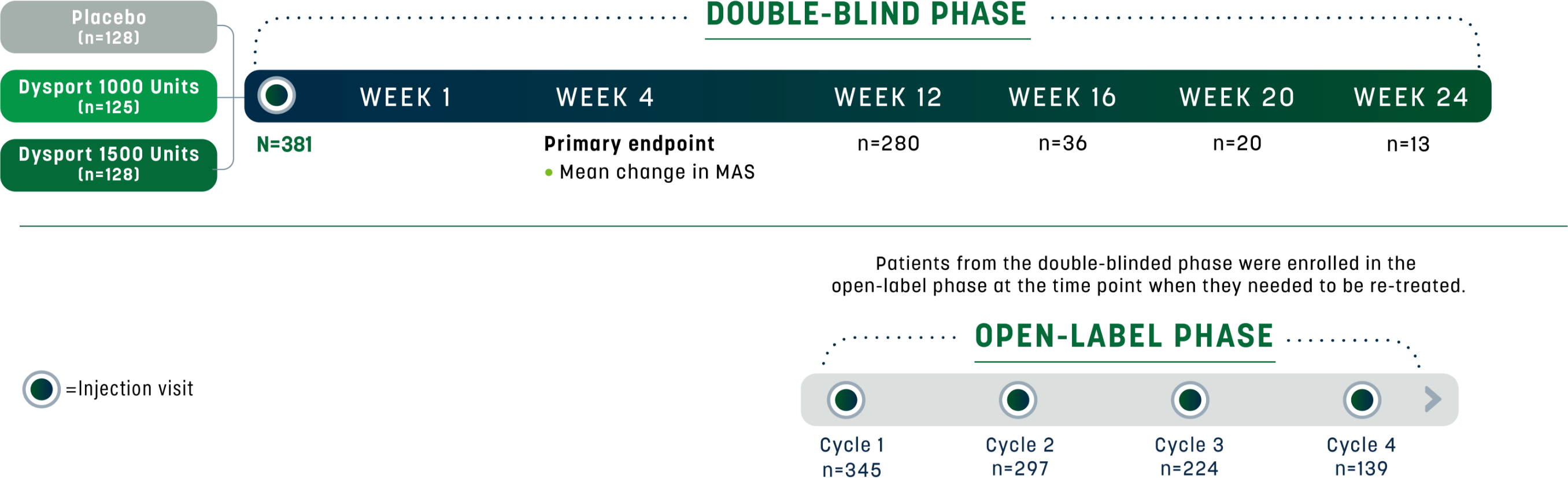
Study design for adult lower limb spasticity
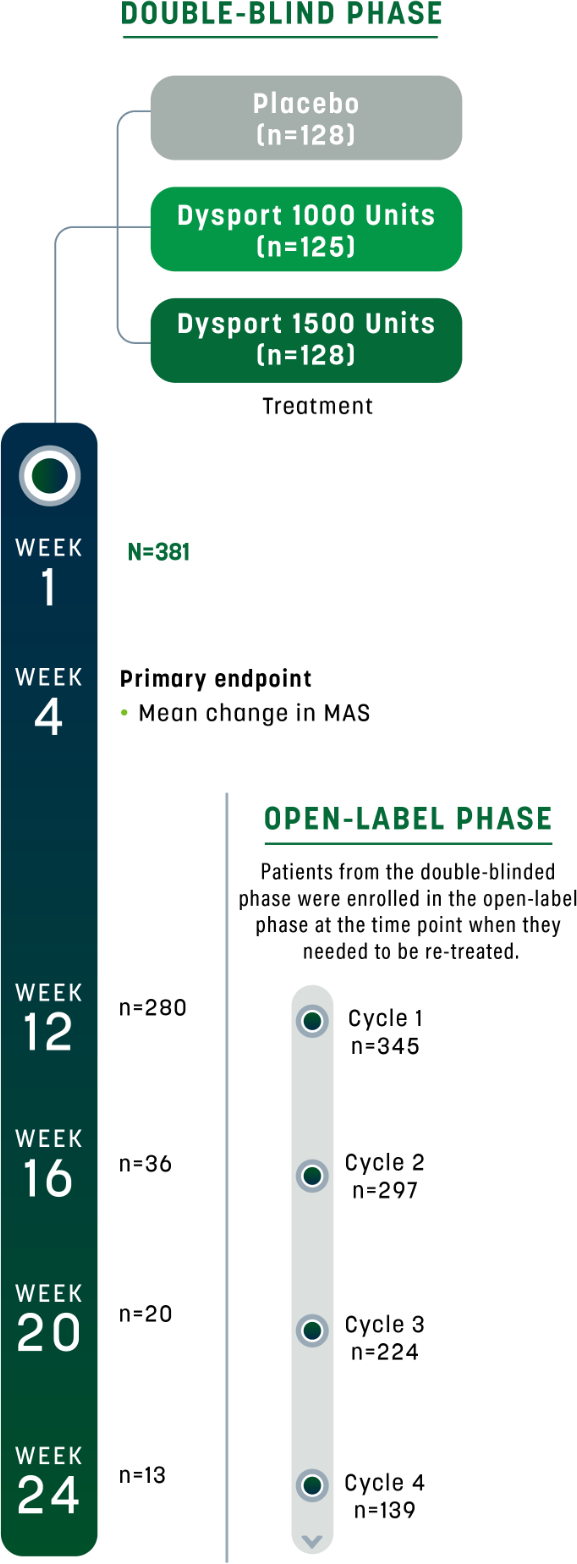
The efficacy and safety of Dysport were evaluated in a randomized, multicenter, double-blind, placebo-controlled study in 381 adults with lower limb spasticity (LLS) who were ≥6 months post-stroke or post-traumatic brain injury. Modified Ashworth Scale (MAS) score was ≥2 in the affected ankle joint for toxin-naive patients, or ≥3 in the affected ankle joint for toxin non-naive patients.1
The primary efficacy endpoint was muscle tone assessed by mean change from baseline in MAS score at the affected ankle joint at Week 4. MAS score at baseline (mean [SD])1,2:
- Placebo: 3.9 (±0.5)
- Dysport 1000 Units: 3.8 (±0.5)
- Dysport 1500 Units: 3.7 (±0.5)
Follow-up assessments occurred at Weeks 1, 4, and 12; follow-up visits were also permitted at Weeks 16, 20, and 24 as needed for re-treatment. After 3 months of on-study treatment, patients were given the opportunity to continue open-label treatment with Dysport. In the open-label phase, patients who were permitted entry from the double-blind study were offered Dysport for ≤4 treatment cycles at ≥12-week intervals. A total of 352 patients were enrolled (14 of the 366 subjects who completed the double-blind study were either not selected by the investigator or declined participation).2
Study design for adult LLS1,2
Study participants included both toxin-naive* and toxin non-naive patients.2

ALL – MAS in affected ankle joint
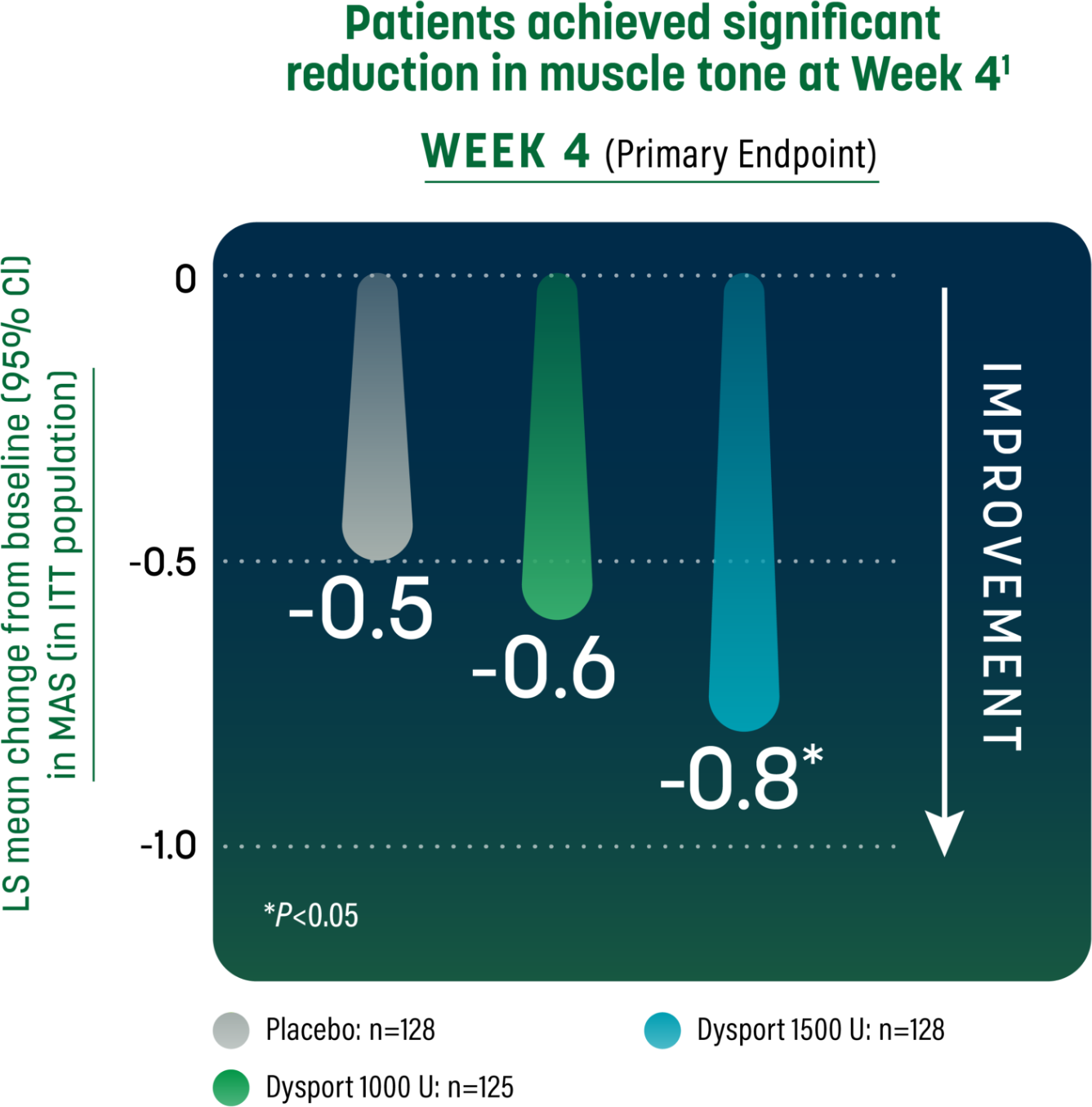
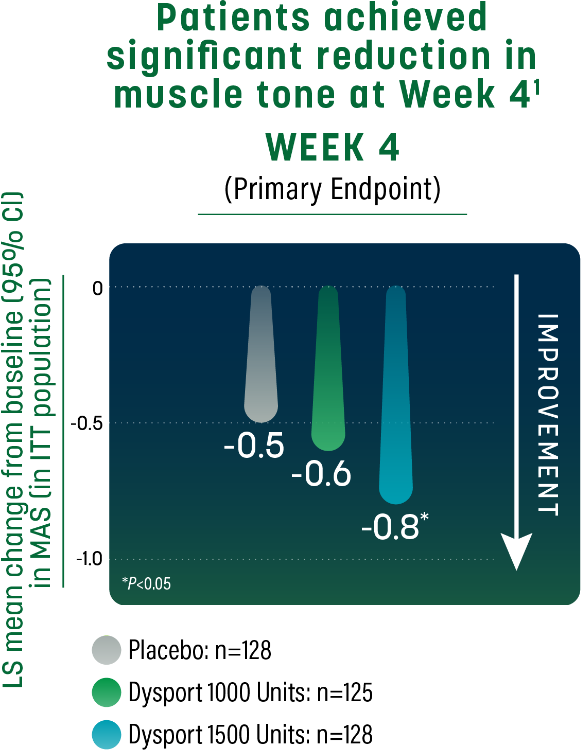
- Patients received Dysport 1000 U, Dysport 1500 U, or placebo. Primary efficacy variable was muscle tone assessed by the MAS at the affected ankle joint at Week 41
- MAS score at baseline (mean [SD]): placebo, 3.9 (0.5); Dysport 1000 Units, 3.8 (0.5); Dysport 1500 Units, 3.7 (0.5)2
- The first secondary endpoint was the PGA at Week 4. LS mean change1:
- – Dysport 1000 Units (n=125): 0.9
- – Dysport 1500 Units (n=128): 0.9
- – Placebo (n=128): 0.7
Study Limitations: Week 12 results may represent chance findings, as multiplicity adjustments were not applied; therefore, the results should be interpreted cautiously.
- Change in MAS at the affected ankle joint through the minimum re-treatment time of 12 weeks2
CI=confidence interval; ITT=intent-to-treat; LS=least squares; PGA=Physician Global Assessment.
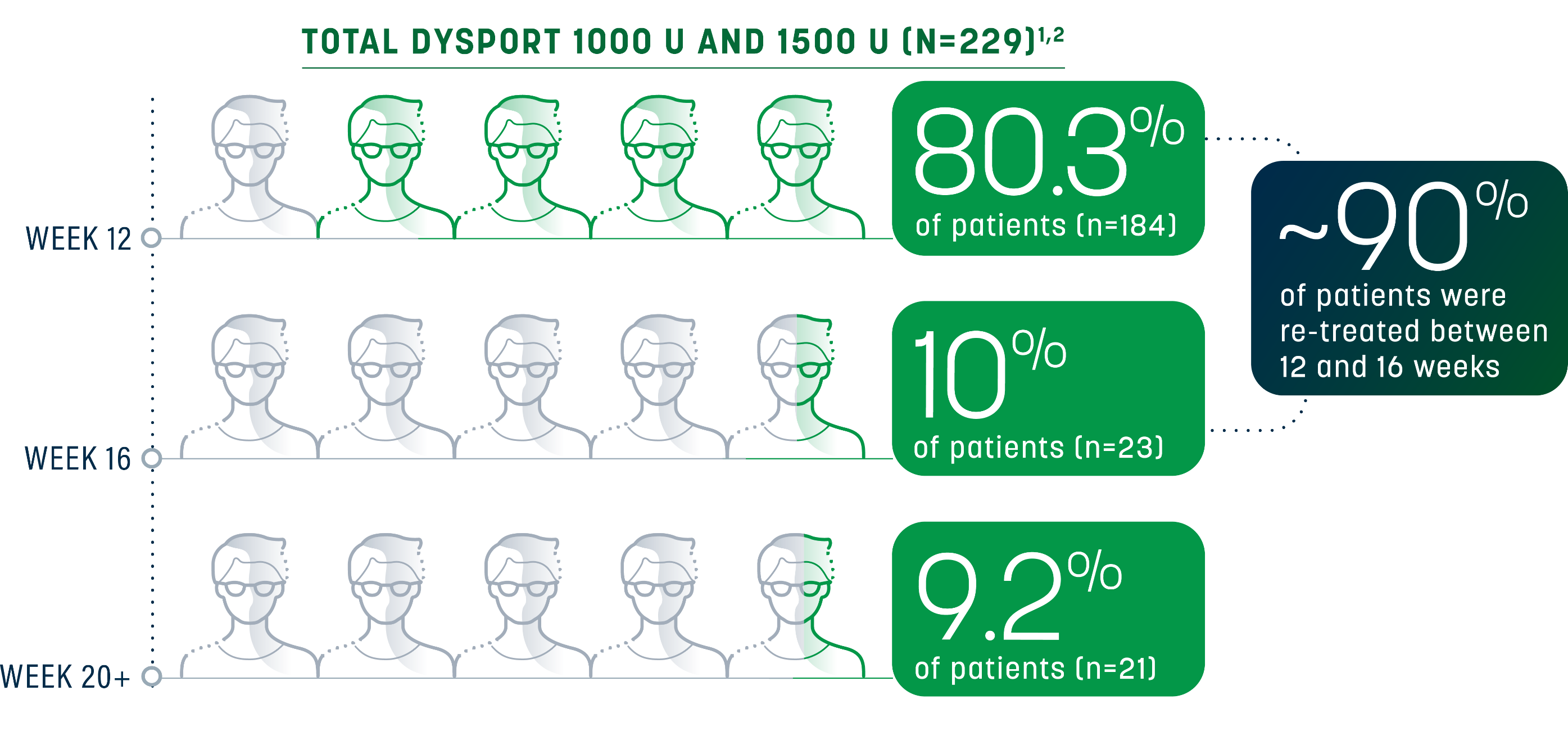
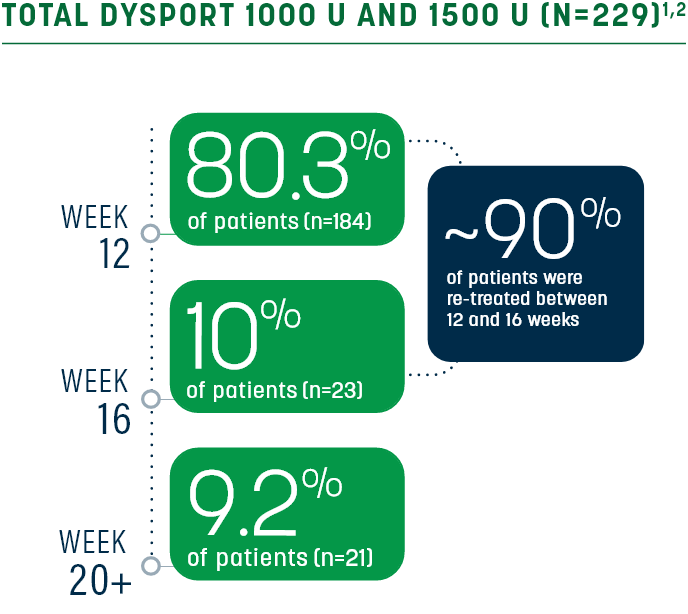
Sustained relief beyond the minimum time to re-treatment
Re-treatment was between 12 and 16 weeks for 90.4% of patients (Dysport 1000 Units, Dysport 1500 Units; n=229); however, some patients had a longer duration of response (20 weeks)1,2
Re-treatment criteria
In the pivotal trials for adult spasticity, need for re-treatment was determined by2:
- No longer demonstrating a decrease from baseline of ≥1 grade in MAS score in the GSC (knee extended)
- No improvement in PGA (ie, a score ≤0)
- No signs of unacceptable safety risk for next treatment cycle
Investigator discretion (based on efficacy and safety criteria) determined the need for re-treatment in patients demonstrating a decrease from baseline of ≥1 grade in MAS score and/or improvement in PGA (ie, a score ≥1).2
Repeat Dysport treatment should be administered no sooner than 12 weeks after the previous injection.1
PGA=Physician Global Assessment; GSC=gastrocnemius-soleus complex.
Learn more about Dysport for adult LLS
INDICATIONS
DYSPORT (abobotulinumtoxinA) for injection is indicated for the treatment of:
- spasticity in patients 2 years of age and older
- cervical dystonia in adults
Please see the Dysport full Prescribing Information, including BOXED WARNING.
IMPORTANT SAFETY INFORMATION
Warning: Distant Spread of Toxin Effect
Postmarketing reports indicate that the effects of DYSPORT and all botulinum toxin products may spread from the area of injection to produce symptoms consistent with botulinum toxin effects. These may include asthenia, generalized muscle weakness, diplopia, blurred vision, ptosis, dysphagia, dysphonia, dysarthria, urinary incontinence and breathing difficulties. These symptoms have been reported hours to weeks after injection. Swallowing and breathing difficulties can be life threatening and there have been reports of death. The risk of symptoms is probably greatest in children treated for spasticity but symptoms can also occur in adults treated for spasticity and other conditions, particularly in those patients who have underlying conditions that would predispose them to these symptoms. In unapproved uses and in approved indications, cases of spread of effect have been reported at doses comparable to or lower than the maximum recommended total dose.
Contraindications
DYSPORT is contraindicated in patients with known hypersensitivity to any botulinum toxin products, cow’s milk protein, or to any of the components in the formulation, or infection at the proposed injection site(s). Serious hypersensitivity reactions including anaphylaxis, serum sickness, urticaria, soft tissue edema, and dyspnea have been reported. If such a serious reaction occurs, discontinue DYSPORT and institute appropriate medical therapy immediately.
Warnings and Precautions
Lack of Interchangeability Between Botulinum Toxin Products
The potency Units of DYSPORT are specific to the preparation and assay method utilized. They are not interchangeable with other preparations of botulinum toxin products and, therefore, units of biological activity of DYSPORT cannot be compared to or converted into units of any other botulinum toxin products assessed with any other specific assay method.
Dysphagia and Breathing Difficulties
Treatment with DYSPORT and other botulinum toxin products can result in swallowing or breathing difficulties. Patients with pre-existing swallowing or breathing difficulties may be more susceptible to these complications. In most cases, this is a consequence of weakening of muscles in the area of injection that are involved in breathing or swallowing. When distant effects occur, additional respiratory muscles may be involved. Deaths as a complication of severe dysphagia have been reported after treatment with botulinum toxin. Dysphagia may persist for several weeks and require use of a feeding tube to maintain adequate nutrition and hydration. Aspiration may result from severe dysphagia and is a particular risk when treating patients in whom swallowing or respiratory function is already compromised. Treatment of cervical dystonia with botulinum toxins may weaken accessory muscles of ventilation, which may result in a critical loss of breathing capacity in patients with respiratory disorders who may have become dependent upon these muscles. Patients treated with botulinum toxin may require immediate medical attention should they develop problems with swallowing, speech, or respiratory disorders. These reactions can occur within hours to weeks after injection with botulinum toxin.
Pre-existing Neuromuscular Disorders
Individuals with peripheral motor neuropathic diseases, amyotrophic lateral sclerosis, or neuromuscular junction disorders (e.g., myasthenia gravis or Lambert-Eaton syndrome) should be monitored particularly closely when given botulinum toxin. Patients with neuromuscular disorders may be at increased risk of clinically significant effects including severe dysphagia and respiratory compromise from typical doses of DYSPORT.
Human Albumin and Transmission of Viral Diseases
This product contains albumin, a derivative of human blood. Based on effective donor screening and product manufacturing processes, it carries an extremely remote risk for transmission of viral diseases and variant Creutzfeldt-Jakob disease (vCJD). There is a theoretical risk for transmission of Creutzfeldt-Jakob disease (CJD), but if that risk actually exists, the risk of transmission would also be considered extremely remote. No cases of transmission of viral diseases, vCJD, or CJD have ever been identified for licensed albumin or albumin contained in other licensed products.
Intradermal Immune Reaction
The possibility of an immune reaction when injected intradermally is unknown. The safety of DYSPORT for the treatment of hyperhidrosis has not been established. DYSPORT is approved only for intramuscular injection.
Pre-existing Conditions at the Injection Site
Caution should be exercised when DYSPORT is used where the targeted muscle shows excessive weakness or atrophy.
Adverse Reactions
- The most common adverse reactions (≥4%) in adults with upper limb spasticity include muscular weakness; in adults with lower limb spasticity (≥5%) include falls, muscular weakness, and pain in extremity
- The most common adverse reactions (≥10%) in pediatric patients with upper limb spasticity include upper respiratory tract infection and pharyngitis; in pediatric patients with lower limb spasticity include nasopharyngitis, cough, and pyrexia
- The most common adverse reactions (≥5%) in adults with cervical dystonia include muscular weakness, dysphagia, dry mouth, injection site discomfort, fatigue, headache, musculoskeletal pain, dysphonia, injection site pain, and eye disorders
Drug Interactions
Co-administration of DYSPORT and aminoglycosides or other agents interfering with neuromuscular transmission (e.g., curare-like agents) should only be performed with caution because the effect of the botulinum toxin may be potentiated. Use of anticholinergic drugs after administration of DYSPORT may potentiate systemic anticholinergic effects such as blurred vision. The effect of administering different botulinum neurotoxins at the same time or within several months of each other is unknown. Excessive weakness may be exacerbated by another administration of botulinum toxin prior to the resolution of the effects of a previously administered botulinum toxin. Excessive weakness may also be exaggerated by administration of a muscle relaxant before and after administration of DYSPORT.
Please see the Dysport full Prescribing Information, including BOXED WARNING.
References:
- Dysport® (abobotulinumtoxinA) [Prescribing Information]. Cambridge, MA: Ipsen Biopharmaceuticals, Inc; September 2023.
- Data on file. Cambridge, MA. Ipsen Biopharmaceuticals, Inc.






